The dethroning process has begun! On March 2, 2021, the governors of Texas and Mississippi declared an end to the mask mandates and lifted all restrictions on businesses. These states are now fully opened! Looks like more states are lining up to follow in their footsteps.
In Dethroning COVID-19 Part 1, we acknowledged that in order to remove the crown from this virus, we need to get honest about it. This starts with being honest about the origins of SARS-CoV-2. We now know the wet market narrative is a farse, and increasingly, the evidence points toward the Wuhan Institute of Virology as the place of origin.
Now, I’m going to go out on a limb here and make an assumption – collectively, we have reached a point where we are no longer willing to let this virus dominate our lives. So, in order to break free from the enslavement that has accompanied this virus, we must ask some difficult questions; questions for which the answers may be too difficult for our psyche to consider. But in order to heal from the trauma of this global pandemic, we have to face these questions head on. So here goes.
What if this pandemic wasn’t really a pandemic after all, but rather a “casedemic” manufactured by faulty testing? What if your businesses were shutdown, your vacations cancelled, your children’s education put on the back burner, your houses of worship closed all because scientists and doctors funded by the WHO, CDC, NIH and NIAID decided to promote a PCR test that was never intended to diagnose a virus? What if there were known cures, readily available, early on in the outbreak, that could have prevented the death of your loved ones? I told you these questions weren’t going to be easy. Brace yourself, the answers may shake the foundation of what you thought you understood about the pandemic, but remember, it’s the TRUTH that sets us free.
Diagnostic Tests
We all remember seeing the footage of people lined up in cars at testing facilities across the nation during the height of the pandemic. I think those images will be etched in our collective conscious for years to come. Odds are, you’ve probably been one of the 334 million Americans tested for the virus. Ever wonder about those tests? What is a PCR test anyway?
The scientific nomenclature for the COVID-19 test is “real-time RT-PCR” which stands for “reverse transcriptase polymerase chain reaction”. The PCR test was developed in 1983 by biochemist Kary Mullis, Ph.D. and in 1993, he was awarded the Nobel Prize in chemistry for it. His invention revolutionized the bio-tech industry. Berkeley professor of molecular and cell biology, David Bilder, Ph.D., stated “PCR revolutionized everything. It really superpowered molecular biology—which then transformed other fields, even distant ones like ecology and evolution. … It’s impossible to overstate PCR’s impact. The ability to generate as much DNA of a specific sequence as you want, starting from a few simple chemicals and some temperature changes—it’s just magical.”(1)
While the PCR test has been an incredible research tool for genomics, it was never meant to be used as a diagnostic tool. Mullis wrote in 2013, “PCR detects a very small segment of the nucleic acid which is part of a virus itself. The specific fragment detected is determined by the somewhat arbitrary choice of DNA primers used which become the ends of the amplified fragment.”(2) He recognized the limitations of PCR as a diagnostic tool, as have many scientists and clinicians.
Early into the pandemic, Dr. David Rasnick, bio-chemist and protease developer stated “You have to have a whopping amount of any organism to cause symptoms…You don’t start with testing; you start with listening to the lungs. I’m skeptical that a PCR test is ever true. It’s a great scientific research tool. It’s a horrible tool for clinical medicine.”(3)
So why did the WHO approve of the PCR test as the diagnostic tool for the pandemic and what are its limitations in diagnosing COVID-19? It appears the PCR test was chosen based on a questionable publication by Eurosurveillance in January 2020. The problems within this publication are numerous starting with the fact the lead authors did not disclose they were on the editorial board of Eurosurveillance. Publication of this Corman-Drosten paper occurred within 24 hours of submission, which means it was virtually impossible for it to have gone through the peer-review process, a standard protocol for publication. Alarmed by the numerous problems within the paper, 22 scientists have since performed a rigorous peer review. The Corman-Drosten paper has had an enormous impact on decisions made by public health officials worldwide, for this reason a peer review was necessary.
Here is a summary of the findings from the 22 scientists published in November 2020 (Corman-Drosten Review Report):
· The PCR protocol for testing SARS-CoV-2 was based on “theoretical” gene sequences. Corman-Drosten did not use an isolated genomic RNA of the virus.
· “To obtain reproducible and comparable results, it is essential to distinctively define the primer pairs” in order to accurately interpret the test results. Corman-Drosten failed to do this. Their protocol design yields 64 possible variations which is not suitable as Standard Operational Protocol (SOP), yet the WHO approved their protocol anyways.
· “In nearly all test procedures worldwide, merely 2 primer matches were used instead of all three. This oversight renders the entire test-protocol useless with regards to delivering accurate test-results of real significance in an ongoing pandemic.”
· The design errors are “so severe that it is highly unlikely that specific amplification of SARS-CoV-2 genetic material will occur using the protocol of the Corman-Drosten paper”.
· A positive RT-PCR test was assumed to mean positive for infection with SARS-CoV-2. This is an errant assumption. A positive RT-PCR test “merely indicates the presence of viral RNA molecules…The Corman-Drosten test was not designed to detect the full-length virus, but only a fragment of the virus…this classifies the test as unsuitable as a diagnostic test for SARS-virus infections.”
· There was no mention of what makes a test positive or negative. “These types of virological diagnostic tests must be based on a SOP, including a validated and fixed number of PCR cycles (Ct value) after which a sample is deemed positive or negative. The maximum reasonably reliable Ct value is 30 cycles. Above a Ct of 35 cycles, rapidly increasing numbers of false positives must be expected. PCR data evaluated as positive after a Ct value of 35 cycles are completely unreliable.”(4)
The most significant limitation of the RT-PCR test is that it cannot distinguish between viral fragments with no infectious potential and the live virus. In fact, studies show that for every one unit increase in Ct value, the odds of having the live virus decrease by 33%.(5) This is astounding! Furthermore, La Scola and Raoult (April 27, 2020) demonstrated that the live virus is found with 100% accuracy at 17 cycles, but anything beyond 34 cycles yields a ZERO percent chance of accurately detecting the live virus.(6)
Now let’s get down to the nitty-gritty.
Multiple studies demonstrate that Ct values above 35 are completely unreliable, yet the WHO, FDA and CDC set the recommended Ct value at 40.(7) WHY? If we have been encouraged to “follow the science”, shouldn’t the WHO also be held to this standard? Absolutely! With experts sounding the alarm regarding the inaccuracies of the PCR test as early as April 2020, why did the WHO wait until January 20th, 2021 to change their recommendations to lower the cycle threshold?(8) Hmmm, what else happened on January 20th, 2021? Oh, that’s right, the inauguration of Joe Biden. Is this a mere coincidence? Perhaps. But if we are trying to get honest about this pandemic, we have to recognize that it was politicized.
The WHO’s decision, at the outset of the pandemic, to set the recommended cycle threshold at 40, produced a “casedemic”. There has never been a SARS-CoV-2 pandemic! Take several deep breaths and let that sink in! If you are still inclined to believe there was a pandemic, a study published in Nature Communications in November 2020 lends more proof that it was merely a “casedemic”. This study found the absence of live virus from the cultures of 300 asymptomatic positive cases identified by the RT-PCR test.(9) In other words, out of the 300 people deemed “infected” with COVID-19 based on the PCR test, researchers found that ZERO were actually infected! Asymptomatic people are in fact, healthy people. It’s time we all agree to stop perpetuating the lie. The truth is ASYMPTOMATIC = HEALTHY!
Look! Magically, the cases have been dropping since the WHO lowered the PCR cycles (Fig 1).
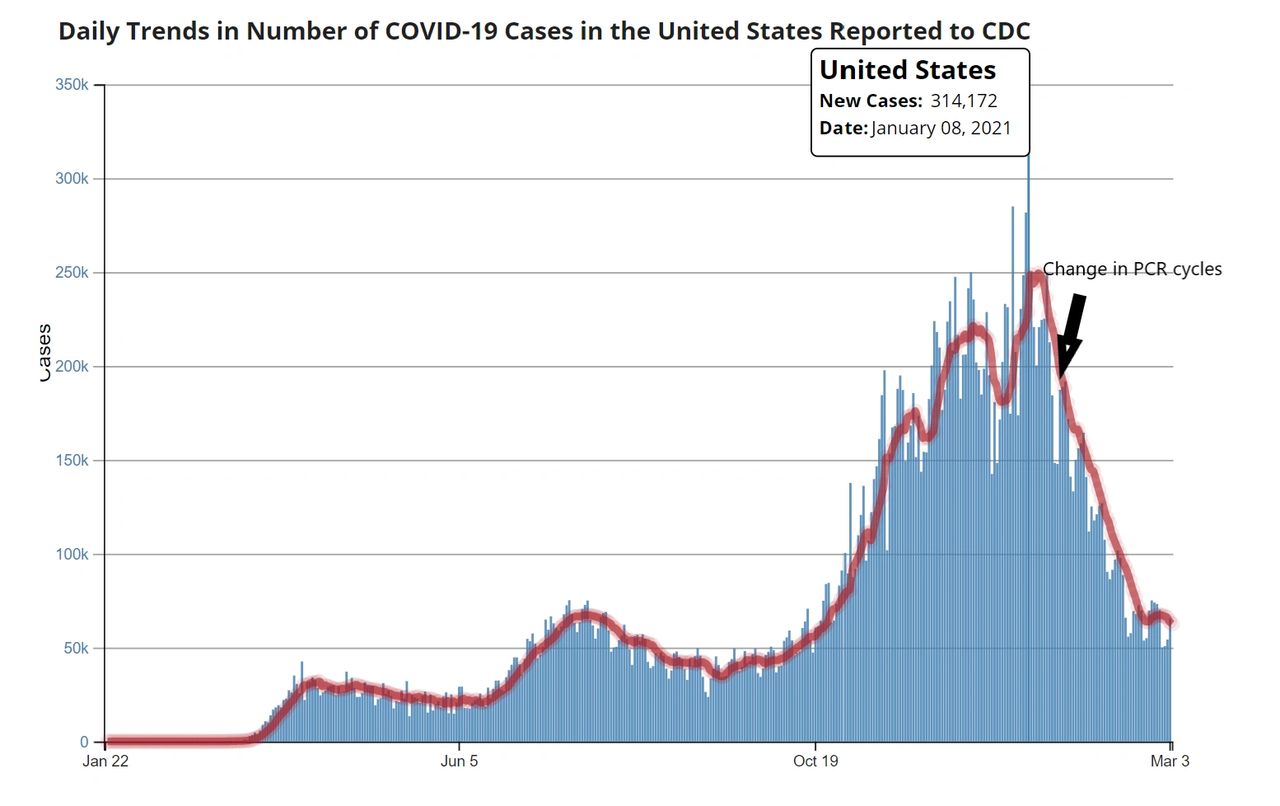
Figure 1. CDC COVID Data Tracker. https://covid.cdc.gov/covid-data-tracker/#trends_dailytrendscases
Treatments
A multitude of heroic physicians from around the world have reported successful treatment protocols for COVID-19 despite receiving intense criticism, censorship, and retribution. Doctors like, Stella Immanuel, M.D., have even boldly declared that there is a cure. A cure? If this is true, then why do we need a vaccine? Let’s examine whether this is true. We’ll start by turning to one of our nation’s leading epidemiologists, a Yale professor, Dr. Harvey Risch, who has authored over 300 peer-reviewed publications.
On July 23, 2020, Dr. Risch, wrote an Opinion piece for Newsweek entitled “The Key to Defeating COVID-19 Already Exists. We Need to Start Using It”. He wrote, “I am usually accustomed to advocating for positions within the mainstream of medicine, so have been flummoxed to find that, in the midst of a crisis, I am fighting for a treatment that the data fully support but which, for reasons having nothing to do with a correct understanding of the science, has been pushed to the sidelines. As a result, tens of thousands of patients with COVID-19 are dying unnecessarily…I am referring, of course, to the medication hydroxycholoroquine.”(10) Dr. Risch also published an article in the American Journal of Epidemiology (May 2020) in which he analyzed five studies that demonstrate “clear and significant benefits” for those treated with hydroxychloroquine (HCQ) in combination with Azithromycin (AZ) and zinc sulfate.
It’s important to note that HCQ has been FDA approved for 65 years and it has shown remarkable success in treating SARS-CoV-2. In the early stages of the outbreak, Dr. Vladimir Zelenko of New York was treating symptomatic patients who were high-risk with 5 days of HCQ + AZ + zinc sulfate. He began treatment for his patients shortly after their symptom onset. By mid-March 2020, he had seen 1,450 patients, 405 of which were considered high-risk and received the treatment protocol. Only six of his patients required hospitalization and two patients died.(11) So with only 2 patients dying out of 1,450 COVID-19 patients, Dr. Zelenko’s patients had a 99.998% survivability rate. Pretty impressive! Perhaps Gov. Cuomo should have consulted with Dr. Zelenko on the best practices for treating COVID-19.
Similarly, physicians in France experienced success in using HCQ + AZ for outpatient treatment of COVID-19. A study out of Marseilles with 42 participants in a controlled but non-randomized or blinded study found astounding results. For patients treated early on in the disease, there was a 50-fold benefit of HCQ + AZ versus the standard of care. When the treatment protocol was given later in the disease process, there was still a 25-fold benefit.(12) Additionally, they found the viral load of SARS-CoV-2 in symptomatic patients cleared within 3 to 6 days of administering the treatment protocol.(13)
Probably most convincing is the meta-analysis of 218 studies investigating the efficacy of HCQ in treating COVID-19 (Figure2). The findings demonstrate that HCQ is an effective treatment, despite what the MSM, CDC, WHO and Dr. Fauci say. In fact, 100% of the early treatment studies report a positive effect from a treatment protocol using HCQ.(14)
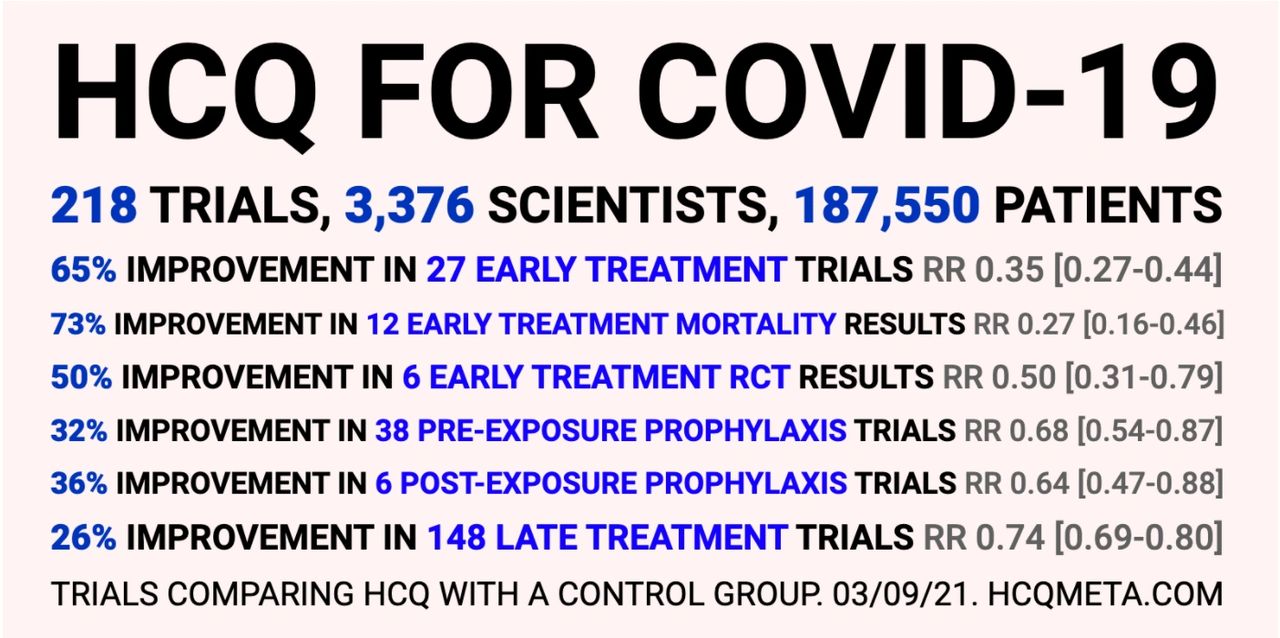
Figure 2. HCQ for COVID-19. https://c19study.com/
These results make me wonder… how many needless deaths occurred because of the public health policies to restrict the use of HCQ, not to mention the biased coverage from MSM? For example, the New York Times only covered negative stories on HCQ. Neil Cavuto of Fox News reported, "If you are in a risky population here, and you are taking this as a preventative treatment ... it will kill you. I cannot stress enough. This will kill you."(15) Does it really Neil? Or were you just fear mongering?
Figure 3 demonstrates that Neil was in fact, just fear mongering. Turns out, the countries that restrict the use of HCQ have the highest case fatality rates. The truth is the exact opposite of what Neil Cavuto exclaimed.
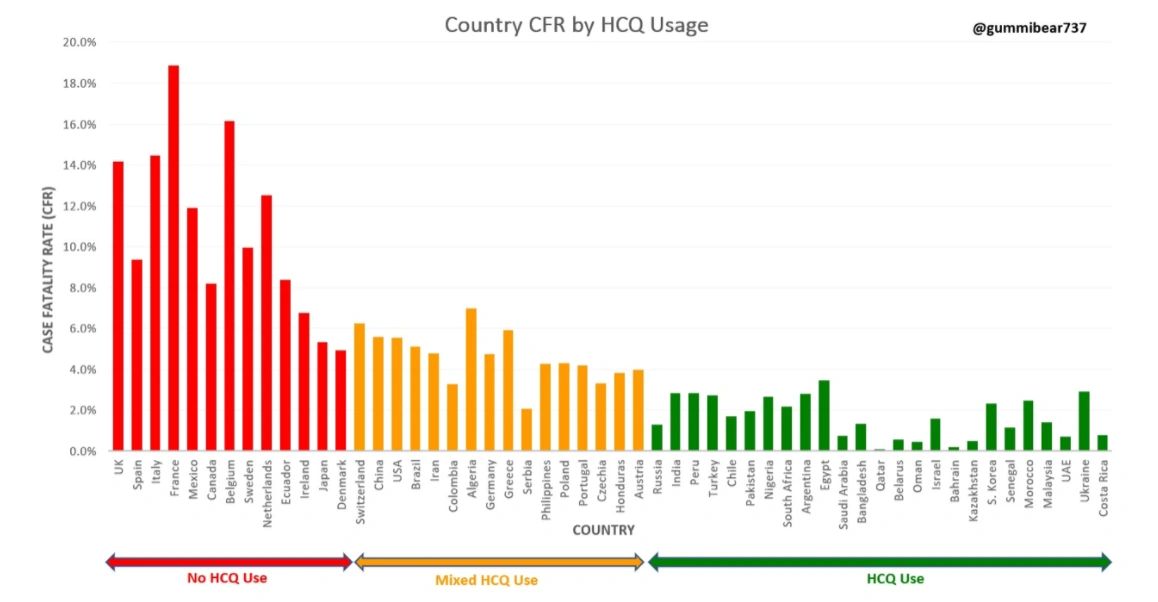
Figure 3. Country CFR by HCQ Usage. Created by Twitter user @gummibear737.
Another drug that has shown positive results in treating COVID-19 is Ivermectin. Dr. Pierre Kory, a critical care physician treating patients with COVID-19, delivered an impassioned testimony before the Senate Homeland Security Committee on December 8, 2020 in which he reported the positive benefits of treating COVID-19 with Ivermectin. One of the clinical studies he cited was a randomized clinical trial (RCT) conducted in Argentina. The RCT found that Ivermectin prevents the replication of SARS-CoV-2. Clinicians administered the drug as a preventive measure to 800 healthcare workers and none tested positive for COVID-19. Whereas, out of 400 healthcare workers that did not receive Ivermectin, 237 were infected with the virus.(16) Dr. Kory testified that the results from research studies show that Ivermectin is effectively a “miracle drug” for treating COVID-19.
Both Ivermectin and HCQ are safe and low-cost treatments for COVID-19. When administered early after symptom onset, they can reduce the length of the disease, reduce the need for hospitalization and reduce the fatality rate of the virus. The question is, if these treatments are so effective, why are they being restricted and censored? I have some theories but I’ll let you draw your own conclusions. In Part 3 of Dethroning COVID-19, we will examine the effectiveness of the mitigation strategies used during the pandemic.
Written by Laura Sanger, Ph.D.
References
1. McDonald, C. (2019). Intolerable Genius: Berkeley’s Most Controversial Nobel Laureate. California Magazine. Retrieved from https://alumni.berkeley.edu/california-magazine/winter-2019/intolerable-genius-berkeleys-most-controversial-nobel-laureate
2. Farber, C (April 7, 2020). Was the COVID-19 Test Meant to Detect a Virus? UndercoverDC. Retrieved from https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/
3. Ibid.
4. Borger, P., Kämmerer, U. et al. (November 27, 2020). Corman-Drosten Review Report. Curated by an International Consortium of Scientists in Life Sciences. Retrieved from https://cormandrostenreview.com
5. T Jefferson, E A Spencer, J Brassey, C Heneghan, Viral cultures for COVID-19 infectious potential assessment – a systematic review, Clinical Infectious Diseases, 2020;, ciaa1764, https://doi.org/10.1093/cid/ciaa1764
6. La Scola, B., Le Bideau, M., Andreani, J. et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis 39, 1059–1061 (2020). https://doi.org/10.1007/s10096-020-03913-9
7. Mercola, J. (February 23, 2021). PCR Testing Saga: Were We Duped? Retrieved from https://childrenshealthdefense.org/defender/pcr-testing-incorrect-use/
8. World Health Organization Medical Alert (January 20, 2021). WHO Information Notice for IVD Users 2020/05: Nucleic Acid Testing (NAT) Technologies that Use Polymerase Chain Reaction (PCR) for Detection of SARS-CoV-2. Retrieved from https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
9. Cao, S., Gan, Y., Wang, C. et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat Commun 11, 5917 (2020). https://doi.org/10.1038/s41467-020-19802-w
10. Risch, H. A. (July 23, 2020). The Key to Defeating COVID-19 Already Exists. We Need to Start Using It. Newsweek. https://www.newsweek.com/key-defeating-covid-19-already-exists-we-need-start-using-it-opinion-1519535
11. Zelenko V. To all medical professionals around the world [letter]. 2020. https://docs.google.com/document/d/1pjgHlqIZuKOziN3txQsN5zz62v3K043pR3DdhEmcos/
12. Risch, H. A. (May 22, 2020). Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients That Should Be Ramped Up Immediately as Key to the Pandemic Crisis. American Journal of Epidemiology, 189 (11), 1218-1226. https://pubmed.ncbi.nlm.nih.gov/32458969/
13. La Scola, B., Raoult D. et al. (April 27, 2020). Viral RNA Load as Determined by Cell Culture as a Management Tool for Discharge of SARS-CoV-2 Patients from Infectious Disease Wards. European Journal of Clinical Microbiology & Infections Diseases, 39, 1059-1061. https://pubmed.ncbi.nlm.nih.gov/32342252/
14. HCQ Meta-Analysis (updated March 9, 2021). HCQ Is Effective for COVID-19 When Used Early. Retrieved from https://hcqmeta.com/
15. Mackey, R. (May 18, 2020). Alarm and Confusion at Fox News as Trump Says He Takes Hydroxychloroquine. The Intercept. Retrieved from https://theintercept.com/2020/05/19/alarm-confusion-fox-news-trump-says-takes-hydroxychloroquine/
16. America’s Frontline Doctors (February 10, 2021). Expanding Use of Ivermectin as Early Treatment for COVID. Retrieved from https://www.americasfrontlinedoctors.com/expanding-use-of-ivermectin-as-early-treatment-forcovid/