As they say, “hindsight is 20/20”. I don’t envy those in public health who were forced to make difficult decisions without understanding important aspects of the SARS-CoV-2 virus. I imagine they were under enormous pressure. It’s somewhat easy to extend grace to public officials who made the wrong decisions but were trying their best to implement mitigation measures that would reduce the severity of the outbreak. It’s more difficult to extend grace to those who abused their power by issuing draconian like mitigation strategies upon their communities. It’s time we take an honest look at whether shutdowns, mask mandates, and “stay at home” orders made a significant difference in “flattening the curve”. Did the benefits outweigh the costs?
To answer this question, we need to keep in mind what we discovered in Dethroning COVID-19 Part 2: Diagnostic Tests and Treatments and that is ASYMPTOMATIC = HEALTHY! The most egregious misnomer of the casedemic was the belief that asymptomatic people can unknowingly spread the virus. This false belief triggered the perceived need for the restrictive mitigation strategies which greatly contributed to the unraveling of civility. How could we have gotten it so wrong?
In the early stages of the outbreak, I think people were erring on the side of caution and drawing conclusions based on scant data that asymptomatic people can spread the virus. Let me provide an example of what I mean by scant data.
Probably the most widely cited study since the outbreak (1,830 citations as of 3/16/21) is an article by Zou et al. (2020). This study was the primary source that fueled the narrative that asymptomatic people transmit the virus. There were two major problems with this study: 1) the data was based on only ONE asymptomatic patient, and 2) they never tested this patient’s contacts to determine whether the virus was transmitted.(1) Despite these major flaws, the findings were cited over and over by scientists around the world to give credence to the belief that asymptomatic people transmit the virus. (I provide a more in-depth look at this study in Analysis of BYU Report: Efficacy of Masks for COVID-19 and Appendix 2 - Scientific Evidence for Asymptomatic Transmission). Is this the “science” referred to when public officials say “follow the science”? Where is the integrity in scientific research these days?
Most of us learned in 6th grade science class that the strength of scientific findings is based upon the design of the research study. To draw conclusions based on one patient is NOT a scientific study, it’s a case study! The scientific community has no business citing Zou et al. (2020) 1,830 times while effectively ignoring other, more robust, studies that contradict these findings. For example, Gao et al. (2020) traced 455 contacts of an asymptomatic carrier of SARS-CoV-2 and found that ZERO of those people who came in contact with the asymptomatic carrier tested positive for COVID-19.(2) In Dethroning COVID-19 Part 2: Diagnostic Tests and Treatments, we reviewed another critical study by Cao et al. (2020) that examined lab cultures from 300 asymptomatic carriers and found no live virus in any of the cultures.(3)
Are you beginning to see the problem with the mantra “follow the science”? I would venture to say that less than 1% of the population have read these three studies I just mentioned. Instead, we have been hoodwinked by the “experts” who supposedly “follow the science”. We just go along with the false narrative that asymptomatic people can transmit the virus. We have bought, hook-line and sinker, the lie that we have been spoon fed. But no more! We will arm ourselves with the truth. We will ask more questions rather than just believing everything we are told. We will do our own research. This is how we will dethrone COVID-19.
Let’s circle back to the first question: Have the benefits of the mitigation strategies outweighed the costs?
Shutdowns
I understand the logic of the shutdowns - if there is a highly contagious virus spreading rapidly across the country, those places that seem to be hotspots for transmission need to lockdown their citizens for the protection of everyone else. I think this made sense to a lot of people, especially Dr. Birx and Dr. Fauci. Remember the messaging in the early days of the outbreak? “15 days to slow the spread”. Well in some states, 15 days turned into 6-9 months of shutdown.
Were these shutdowns effective at lowering the mortality rate? Let’s contrast the mortality rates of the states that imposed strict mitigation strategies, such as “stay at home” orders, mask mandates, and closure of all non-essential businesses versus those states that didn’t. Surprisingly, there was only one state in the U.S. that did not impose any COVID-19 restrictions – South Dakota. There were no mask mandates, no church closures, no “stay at home” orders, no business closures and school districts were able to independently determine whether in-person learning was viable for their communities. The table below demonstrates that there was not a noticeable difference in mortality rates between South Dakota and the other states that implemented more restrictive mitigation strategies. While
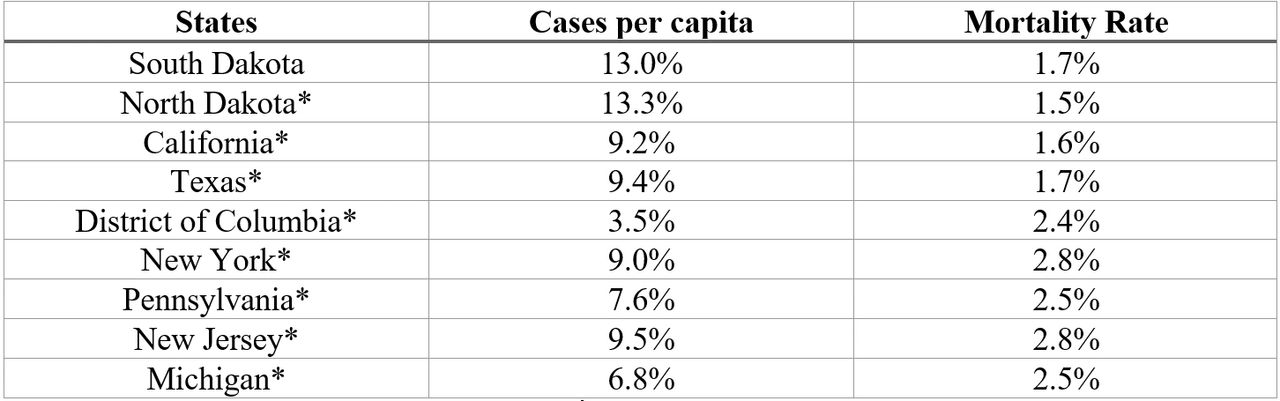
Statistics retrieved from https://covidusa.net/
* mask mandates, “stay at home” orders, & non-essential business closures.
the cases per capita in South Dakota were on the high side compared to most the other states, the mortality rate was lower than many of the states that were more restrictive. It’s important we consider the big picture because these mortality rates don’t account for the deaths caused by the restrictive mitigation strategies i.e., suicides, domestic violence, child abuse, untreated medical conditions, and “despair deaths”. In fact, South Dakota did not see an increase in suicides in 2020 as compared to 2019.(4) This is not true of other states that imposed restrictions. In the coming months and years, “despair deaths” alone are likely to surpass COVID-19 deaths due to the devastating economic impact of the shutdowns. Small businesses were especially hit hard.
Research collected by Yelp in September 2020 estimated that 60% of the businesses that were forced to temporarily close will never re-open because they weren’t able to withstand the loss of revenue.(5) At the height of the casedemic, 20.5 million Americans were unemployed. The true impact of the shutdown is hard to quantify, but we can turn to research conducted by Roelfs et al. (2011) to get a sense of how many “despair deaths” may result from the shutdowns.
Roelfs et al. (2011) conducted a random effects meta-analysis to assess the association between unemployment and mortality among working-age individuals. Their sample size was 20 million people. They found that “unemployment was associated with an increased mortality risk for those in their early and middle careers…The risk for death was highest during the first 10 years of follow-up. The risk of death for unemployed persons was 63% higher than the risk of death for employed persons.”(6)
WOW!!! Did you catch that?
Let me put it in perspective - For people in their early to middle careers, the infection fatality rate of COVID-19 is 0.02% - 0.5%, so the chance of survival is 99.98% - 99.5% should they get infected with the virus (see SARS-CoV-2 Vaccine: Make an Informed Decision for infection fatality rate). But the shutdowns and subsequent unemployment placed these same people at a 63% higher risk of death than their counterparts in regions of the country without restrictive mitigation strategies!!!
This is tragic!
I mentioned that hindsight is 20/20, but only if we are willing to see the truth. If we never examine the costs of the restrictive mitigation strategies, we will blindly accept more shutdowns.
Masks
Let’s review all the mixed messaging on masks since the outbreak began, compliments of Dr. Fauci.
On March 8, 2020, Dr. Fauci explained, “The masks are important for someone who is infected to prevent them from infecting someone else…right now in America, people should not be wearing masks. When you are in the middle of an outbreak, wearing a mask, it may make people feel a little bit better, it might even block a droplet but it’s not providing the perfect protection that people think that it is.”(7)
On April 3, 2020, Dr. Fauci said, “Data indicate that people who are without the symptoms at all can transmit the virus… putting a mask on yourself is more to prevent you from infecting someone else… we are each protecting each other because the data is that it is more efficient to prevent transmitting to others than it is to prevent transmission to yourself.”(8)
On May 27, 2020, Dr. Fauci declared, “I wear it [masks] for the reason that I believe it is effective, it’s not 100% effective but it’s sort of having respect for another person and that person having respect for you. You wear a mask, they wear a mask, you protect each other. I do it when I am in the public…because I want to make it be a symbol for other people to see that that is the kind of thing you should be doing.”(9)
On January 25, 2021, Dr. Fauci stated, “So if you have a physical covering with one layer, you put another layer on, it just makes common sense that it likely would be more effective.”(10)
Common sense? Someone who has been telling us to “follow the science” is now telling us to use common sense? Is it really common sense to wear two masks? I guess if you don’t care about breathing oxygen deficient air it is.
Common sense says we need to breathe oxygen to stay alive. Common sense says that healthy people should not be wearing masks. Common sense says only those who are infectious or in a high-risk category should be wearing masks.
Dr. Judy Mikovits points out that wearing a mask forces you to breathe in the carbon dioxide your body is trying to get rid of. When inhaling, a person breathes in 21% oxygen and 0.04% carbon dioxide. When exhaling, a person releases 16% oxygen and 4% carbon dioxide.(11) If you notice, there is a 100-fold increase in carbon dioxide from inhaling to exhaling. So, when you wear a mask, you are breathing the air that is trapped inside the mask which has 5% less oxygen and 100 times more carbon dioxide. This is NOT healthy for us!
OSHA’s Respiratory Protection Standard states “human beings must breathe oxygen . . . to survive, and begin to suffer adverse health effects when the oxygen level of their breathing air drops below [19.5 percent oxygen]. Below 19.5 percent oxygen… air is considered oxygen-deficient. At concentrations of 16 to 19.5 percent, workers engaged in any form of exertion can rapidly become symptomatic as their tissues fail to obtain the oxygen necessary to function properly”.(12)
Lower oxygen levels weaken the immune system and trigger latent viruses within our body which then causes illness. It’s a bit ironic that people report feeling “safer” when wearing a mask because truthfully, they are more susceptible to getting infected with COVID-19, not only because of oxygen deficiency, but for a host of other reasons listed below.
· People who have received flu vaccines are 36% more likely to get infected with a coronavirus if they wear masks.(13)
· Mask usage produces humidity around the mouth which becomes the perfect scenario for bacteria and viruses to grow. By trapping the virus inside the mask and breathing it in, it increases the viral load in the lungs and nasal passages.(14)
· Cloth masks allow 97% of virus particles through and surgical masks allow 44% of virus particles through. Researchers warn people from using cloth masks because of “moisture retention, reuse of cloth masks, and poor filtration may result in increased risk of infection.”(15)
· The airflow from masks pushes air up into the eyes which activates a separate immune system (ocular immune system) than the nasal passageways (mucosal immune system). Mask usage taxes multiple immune systems at once.(16)
· Dr. Daniel Erickson explains it plainly. “Wearing a mask reduces your bacteria flora; it doesn’t allow you to interact with other viruses and bacteria and your own bacteria (which is your friend) end up disappearing which make you more susceptible to other diseases. You are more susceptible to get ‘opportunistic infections’ which are infections that hope you don’t have the ‘good bugs’ or bacteria to fight them off. The building blocks of your immune system is virus and bacteria, end of story”.(17)
The primary narrative that led to mask mandates was that asymptomatic people can spread the virus. This simply is not true! Remember our new mantra based on robust scientific studies? ASYMPTOMATIC = HEALTHY.
Ask yourself this simple question, when have masks ever been required during other viral outbreaks? That’s right, NEVER! And there is good reason for that. Masks do not stop a virus particle from penetrating, despite what the CDC, WHO and NIH have told us. It’s like trying to block a grain of sand using a chain link fence. Of course, the CDC and NIH used convincing arguments such as, the virus attaches to droplets which are much larger in size therefore they are blocked by masks. But this is not true either. Dr. Fauci and others will quote scientific studies conducted by the NIH to back this claim, but when you take the time to read the study they reference, it’s quite eye-opening.
The NIH study conducted to demonstrate that cloth masks reduce the penetration of droplets was a study that did not even use cloth masks! Instead, the NIH researchers placed a wet washcloth over the participant’s mouth as they measured the reduction in droplets produced by speech.(18) What? A wet washcloth? Now how many people have you seen walking around town wearing a wet washcloth over their mouth? The research design of this study was clearly flawed and yet it has been touted as the scientific proof that masks work to block the virus.
An article in the New England Journal of Medicine from a group of physicians associated with Harvard Medical School states, “we know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.”(19)
Conclusion
In this 3 Part Series, we have discovered many shocking revelations. These truths have the ability to demolish the false narratives we have been conditioned to believe over the past year. We must keep these truths at the forefront of our mind so that they can season our conversations.
· COVID-19 is a bioengineered virus.
· COVID-19 most likely originated from the Wuhan Institute of Virology.
· COVID-19 was not a global pandemic but a global casedemic.
· The PCR tests are 100% accurate at 17 cycles, but completely inaccurate at 40 cycles (WHO recommended 40 cycles until January 20, 2021, at which time they suggested lowering the cycles).
· HCQ and Ivermectin cure COVID-19 but are restricted in many states.
· Doctors and scientists that spoke out about known cures were censored and/or fired from their jobs.
· Restrictive mitigation strategies such as, mask mandates, shutdowns, and “stay-at-home” orders do not reduce mortality rates for COVID-19.
· The economic hardships created by the shutdowns are likely to produce more deaths than COVID-19.
· Mask mandates do not reduce the transmission of the virus in the community.
· Mask usage weakens the immune system and makes people more susceptible to infection.
Mark Twain said “It’s easier to fool people than convince them that they have been fooled.”
Don’t let yourself be fooled any longer! Dethrone COVID-19! Remove the power it has over your life so you are No Longer Enslaved!
Written by Laura Sanger, Ph.D.
References
1. Zou, L. et al. (March 19, 2020). SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. New England Journal of Medicine 382, 1177–1179.
2. Gao, M. (2020, May 13). A Study of Infectivity of Asymptomatic SARS-CoV-2 Carriers. Respiratory Medicine. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
3. Cao, S., Gan, Y., Wang, C. et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nature Communications 11, 5917 (2020). https://doi.org/10.1038/s41467-020-19802-w
4. Noem, K. (December 7, 2020). South Dakota’s Balanced Covid Response. Wall Street Journal Opinion. Retrieved from https://www.wsj.com/articles/south-dakotas-balanced-covid-response-11607381485
5. Sardana, S. (September 17, 2020). Yelp Says 60% of US Businesses That Closed Due to COVID-10 Won’t Reopen. Markets Insider. Retrieved from https://markets.businessinsider.com/news/stocks/yelp-business-closures-permanent-covid-report-2020-9-1029598577?op=1
6. Roelfs D. J., Shor, E., Davidson, K. W., Schwartz, J. E. (March 2011). Losing Life and Livelihood: A systematic review and meta-analysis of unemployment and all-cause mortality. Social Science & Medicine (72), pp. 840-854.
7. Fauci, A. (2020, March 8). Dr. Anthony Fauci Talks with Dr. Jon LaPook About COVID-19. [60 Minutes]. Retrieved https://www.youtube.com/watch?v=PRa6t_e7dgI
8. Fauci, A. (2020, April 3). What Dr. Fauci Wants You To Know About Face Masks and Staying Home as Virus Spreads. [PBS News Hour]. Retrieved from https://www.youtube.com/watch?v=CXjRfBa0pYE
9. Fauci, A. (2020, May 27). Second Wave Isn’t Inevitable If We Do This. [CNN]. Retrieved from https://www.youtube.com/watch?v=vGj5XrPP6Mw
10. Steig, C. (January 25, 2021). Dr Fauci: Double-Masking Makes ‘Common Sense’ and is Likely More Effective. CNBC. Retrieved from https://www.cnbc.com/2021/01/25/dr-fauci-double-mask-during-covid-makes-common-sense-more-effective.html
11. Mikovits, J. A. and Heckenlively, K. (2020). The Case Against Masks. New York, NY: Skyhorse Publishing.
12. Fairfax, R. E. (2007, April 2). Letter to Mr. William Costello from the Directorate of Enforcement Programs OSHA. Retrieved from https://www.osha.gov/laws-regs/standardinterpretations/2007-04-02-0
13. Wolff, G. (2020, January 10). Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-208 influenza season. Vaccine, 38(2), pp. 350-354.
14. Mikovits, J. A. and Heckenlively, K. (2020). The Case Against Masks. New York, NY: Skyhorse Publishing.
15. MacIntyre, C. R. et. al. (2015). A cluster randomized trial of cloth masks compared with medical masks in healthcare workers. BMJ Open, 5(4).
16. Mikovits, J. A. (March 3, 2021). ReOpen San Diego Presents Dr. Judy Mikovits [Rumble]. Retrieved from https://rumble.com/veetif-reopen-san-diego-presents-dr.-judy-mikovits.html
17. Dr. Daniel Erickson and Dr. Artin Massih press briefing (2020). Retrieved from https://londonreal.tv/is-coronavirus-a-plandemic-exposing-the-truth-behind-americas-covid-19-strategy-dr-judy-mikovits/
18. Anfinrud, P., Stadnytskyi, V., Bax, C. E. & Bax, A. (2020). Visualizing Speech-Generated Oral Fluid Droplets with Laser Light Scattering. New England Journal of Medicine 382, 2061–2063.
19. Klompas, M, Morris, C. A., Sinclair, J., Pearson, M., and Shenoy, E. S. (2020, April 1). Universal Masking in Hospitals in the COVID-19 Era. New England Journal of Medicine, 382, e63. Retrieved from https://www.nejm.org/doi/full/10.1056/NEJMp2006372