- Evolving Information Regarding the Spread of the Virus
- Early on in the pandemic the CDC website stated on 3/26/20: “There is much to learn about the novel coronavirus (SARS-CoV-2) that causes coronavirus disease 2019 (COVID-19). Based on what is currently known about COVID-19, spread from person-to-person of this virus happens most frequently among close contacts (within about 6 feet). This type of transmission occurs via respiratory droplets. On the other hand, transmission of novel coronavirus to persons from surfaces contaminated with the virus has not been documented. Recent studies indicate that people who are infected but do not have symptoms likely also play a role in the spread of COVID-19. Transmission of coronavirus occurs much more commonly through respiratory droplets than through fomites. Current evidence suggests that SARS-CoV-2 may remain viable for hours to days on surfaces made from a variety of materials. Cleaning of visibly dirty surfaces followed by disinfection is a best practice measure for prevention of COVID-19 and other viral respiratory illnesses in households and community settings.”(1)
- May 22, 2020 the CDC website stated: “It may be possible that a person can get COVID-19 by touching a surface or object that has the virus on it and then touching their own mouth, nose, or possibly their eyes. This is not thought to be the main way the virus spreads, but we are still learning more about how this virus spreads.”(2)
- Dr. John Whyte, chief medical officer for WebMD called the CDC changes an “important step in clarifying how the virus is spread, especially as we gain new information. It also may help reduce anxiety and stress. Many people were concerned that by simply touching an object they may get coronavirus and that’s simply not the case. Even when a virus may stay on a surface, it doesn’t mean that it’s actually infectious.”(3)
- June 9, 2020 – WHO’s Head of Emerging Diseases, Dr. Maria Van Kerkhove, reported that the spread of COVID-19 by patients who are asymptomatic is “very rare”. She stated “from the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual. We have a number of reports from countries who are doing very detailed contact tracing. They’re following asymptomatic cases. They’re following contacts. And they’re not finding secondary transmission onward. It’s very rare.”(4) This aligns with common sense regarding public health. Dr’s have told us for years that we are contagious if we have a fever, cough or the drainage of mucus, but when these symptoms have cleared, we are no longer contagious. The narrative that asymptomatic people were spreading COVID-19 fed into the agenda of lockdown, social distancing and wearing of masks. People’s lives have been ruined because of this false narrative.
- May 13, 2020 – Chinese researchers found no transmission of an asymptomatic carrier of COVID-19. An asymptomatic 22 year-old woman presented to the hospital for congenital heart disease and was tested for COVID-19. She tested positive so researchers traced her contacts for 5 days prior to testing. They identified 455 people, COVID-19 tests were given to all her contacts and zero came back positive.(5)
- Inaccurate Virus Models
- The COVID Act Now models have been grossly inaccurate and have caused state governments to overreact. This model comes from a team of researchers at Imperial College London, led by Britain’s leading epidemiologist, Neil Ferguson (who has since resigned because he was caught violating his own lockdown orders when his lover visited him). Critics have said that Ferguson has not been transparent in the coding of their data. Other researchers argue that the model is flawed with “incorrect assumptions”.(6) Unfortunately, state officials relied on this model to impose lockdowns.
- New York Times article: Ferguson released a doomsday prediction in his report that 2.2 million Americans would die from COVID-19 if nothing was done. In order “to curb the epidemic, there would need to be drastic restrictions on work, school and social gatherings for periods of time until a vaccine was available, which could take 18 months. They cautioned that such steps carried enormous costs that could also affect people’s health, but concluded they were the only viable strategy at the current time”.(7)
- Michigan Gov. Whitmer cited COVID Act Now when declaring Michigan would see more than 7 million people infected, 1 million hospitalized and 460,000 deaths if the state did nothing to flatten the curve.(8) As of 5/14/20, Michigan has had 49,582 cases as listed by Michigan.gov coronavirus statistics. This is a far cry from 7 million.
- New York Gov. Cuomo on March 27th “all the projections say you could have an apex needing 120,000 beds and about 40,000 ventilators…We are following the data and the science and that’s what the data and the science says.”(9) New York only used about 25% of that total.
- The COVID Act Now models have been grossly inaccurate and have caused state governments to overreact. This model comes from a team of researchers at Imperial College London, led by Britain’s leading epidemiologist, Neil Ferguson (who has since resigned because he was caught violating his own lockdown orders when his lover visited him). Critics have said that Ferguson has not been transparent in the coding of their data. Other researchers argue that the model is flawed with “incorrect assumptions”.(6) Unfortunately, state officials relied on this model to impose lockdowns.
- Inflated Mortality Rates
- Dr. Birx stated in WH daily press briefing on April 7, 2020 regarding COVID-19 mortality rates “We are taking a very liberal approach to mortality…if someone has a pre-existing illness…but they die with COVID-19, we count that as a COVID-19 death”.(10) Is Dr. Birx encouraging the manipulation of data to misrepresent the truth?
- In an April 27th press conference, Illinois State Health Director, Dr. Ngozi Ezike, explained how they are applying the “very liberal” approach of assigning death codes for COVID-19. “I just want to be clear in terms of the definition of people dying of COVID. The case definition is very simplistic. It means at the time of death, it was a COVID positive diagnosis. That means if you were in hospice and already given a few weeks to live, and then you were also found to have COVID, that would be counted as a COVID death. It means, technically even if you died of a clear alternative cause but you had COVID at the same time, it’s still listed as a COVID death. Everyone who is listed as a COVID death, does not mean that was the cause of the death, but they had COVID at the time of death.”(11) How many other states are coding COVID-19 deaths in this manner? This certainly would inflate the mortality rate.
- Infection Fatality Rate (IFR)
- In March, the CDC predicted an IFR of 0.8% leaving 1.7 million Americans dead. At about the same time, the researchers from the Imperial College of London based their doomsday prediction of 2.2 million Americans dead based on an IFR of 0.9%. These predictions were not altered despite data provided from Stanford researchers starting April 17th, 2020. The research findings have become even more robust since April.
- Dr. John Ioannidis of Stanford University conducted a meta-analysis of 12 IFR research studies. The findings were reported on May 13, 2020: “The infection fatality rate (IFR), the probability of dying for a person who is infected, in one of the most critical and most contested features of the coronavirus disease 2019 (COVID-19) pandemic. The expected total mortality burden of COVID-19 is directly related to the IFR. Moreover, justification for various non-pharmacological public health interventions depends crucially on the IFR. Some aggressive interventions that potentially induce also more pronounced collateral harms may be considered appropriate, if IFR is high. Conversely, the same measures may fall short of acceptable risk-benefit thresholds, if the IFR is low…Interestingly, despite their differences in design, execution, and analysis, most studies provide IFR point estimates that are within a relatively narrow range. Seven of the 12 inferred IFRs are in the range 0.07 to 0.20…which are similar to IFR values for the seasonal influenza.”(12)
- Metrics for Case Counts
- Virginia – State Health Department issued a change to their case count guidelines on May 1, 2020. “We have made the change to report the number of people tested per day rather than the number of unique people who have been tested at any point during the response. We know individual people, especially healthcare workers and those in high-risk settings, may be tested more than once over time.”(13) So rather than count the number of tests based on unique people, if an individual is tested multiple times, each of those tests is counted. Joe Macenka, a spokesman for Virginia’s COVID-19 Joint Information Command stated “if a person is tested on different days, those tests are counted as separate. Repeat positive cases are counted as separate cases only if the tests occur on different days. If [a Virginia resident] tested Monday and Tuesday and both are positive, that’s two positives.”(14)
- Utah – Case counts as of July 29 were 39,194. The total amount of people tested were 518,191, but yet 616,512 tests were reported. This means there were 98,321 more tests conducted than people tested. Utah Department of Health states they follow case definitions from the CDC. If we look at Figure 2 below, the CDC does not provide any information about how to distinguish an existing case from a new case. This suggests that Utah may be applying the same standards as Virginia, each test reported as positive may be counted as a new case.

Figure 1. Overview of COVID-19 Surveillance. https://coronavirus.utah.gov/case-counts/
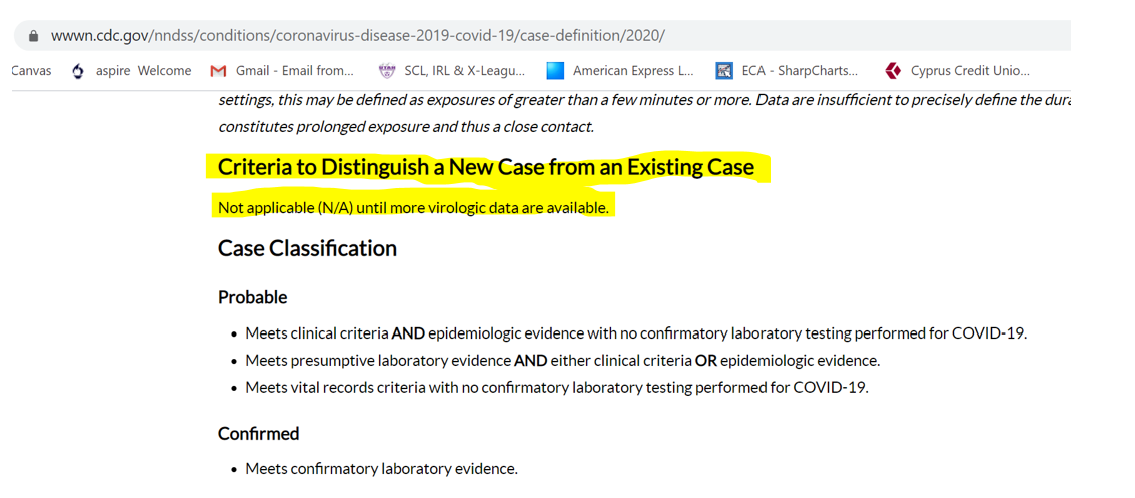
Figure 2. CDC Case Definitions modified by Laura Sanger, Ph.D. https://wwwn.cdc.gov/nndss/conditions/coronavirus-disease-2019-covid-19/case-definition/2020/
Written by Laura Sanger, Ph.D.
References
- Cleaning and Disinfection for Households (2020, March 26). Coronovirus Disease 2019. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cleaning-disinfection.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fprepare%2Fcleaning-disinfection.html
- How COVID-19 Spreads (2020, May 22). Coronovirus Disease 2019. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html
- Farber, M. (2020, May 20). CDC Now Says Coronavirus ‘Does Not Spread Easily’ Via Contaminated Surfaces. Fox News. Retrieved from https://www.foxnews.com/health/cdc-now-says-coronavirus-does-not-spread-easily-via-contaminated-surfaces
- Nguyen Ly, M. (2020, June 9). WHO: Asymptomatic Spread of CCP Virus ‘Very Rare’. Epoch Times. Retrieved from https://www.theepochtimes.com/who-asymptomatic-spread-of-ccp-virus-very-rare_3381512.html#
- Gao, M. (2020, May 13). A Study of Infectivity of Asymptomatic SARS-CoV-2 Carriers. Respiratory Medicine. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
- Osburn, M (2020, March 25). Inaccurate Virus Models Are Panicking Officials into Ill-Advised Lockdowns. The Federalist. Retrieved https://thefederalist.com/2020/03/25/inaccurate-virus-models-are-panicking-officials-into-ill-advised-lockdowns/
- Fink, S. (2020, March 16). White House Takes New Line After Dire Report on Death Toll. New York Times. Retrieved from https://www.nytimes.com/2020/03/16/us/coronavirus-fatality-rate-white-house.html
- Osburn, M (2020, March 25). Inaccurate Virus Models Are Panicking Officials into Ill-Advised Lockdowns. The Federalist. Retrieved https://thefederalist.com/2020/03/25/inaccurate-virus-models-are-panicking-officials-into-ill-advised-lockdowns/
- Ingraham, L. (2020, May 4). Ingraham: The ‘Experts’ Strike Again. [Fox News]. https://www.youtube.com/watch?v=5iPihogbh3o&t=250s
- Prestigiacomo, A. (2020, April 7). Watch: Dr. Birx: We Have ‘Very Liberal’ Recording of COVID Deaths; If They Test Positive, ‘We are Counting That’. The Daily Wire. Retrieved from https://www.dailywire.com/news/watch-dr-birx-we-have-very-liberal-recording-of-covid-deaths-if-they-test-positive-we-are-counting-that
- Thrivetime Show (April 27, 2020). Dr. Ngozi Ezike: How COVID Deaths are Classified. [Thrivetime Show: Business School without the BS]. https://www.youtube.com/watch?v=Tw9Ci2PZKZg
- Ionnidis, J. (2020, May 13). The Infection Fatality Rates of COVID-19 Inferred from Seroprevalence Data. medRxIV. Retrieved from https://www.medrxiv.org/content/10.1101/2020.05.13.20101253v2.full.pdf+html
- May 1 Data Improvements (2020, May 2). Virginia Department of Health. Retrieved from https://www.vdh.virginia.gov/coronavirus/2020/05/02/data-improvements/
- Payne, D. (2020, May 4). Virginia to Begin Double-Counting Multiple Positive Coronavirus Cases. Just the News. Retrieved from https://justthenews.com/politics-policy/coronavirus/virginia-begin-double-counting-positive-coronavirus-cases